
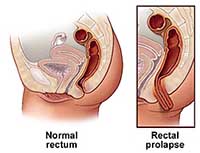
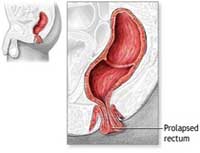
Rectal prolapse is a condition in which the rectum (a portion of the colon) looses its internal support and protrudes from the anus. Rectal prolapse may be internal but in advanced stages, it can be seen or felt outside the body. When this occurs, it is referred to as a complete rectal prolapse.
Why does it occur ?
Rectal prolapse can occur due to a lifelong habit of straining during bowel movement, hereditary factors, stresses due to childbirth or as part of the aging process when pelvic and anal sphincter muscles weaken. It occurs in women more often than men and its symptoms can often mimic those of hemorrhoids.
Stool softeners or other treatments for constipation may help but will not reverse the prolapse once it has developed. With complete rectal prolapse, incontinence (uncontrolled leakage of stool) can occur and surgical treatment may become necessary.
There are three chief conditions which come under the title rectal prolapse : -
 Full-Thickness rectal prolapse describes the entire rectum protruding through the anus
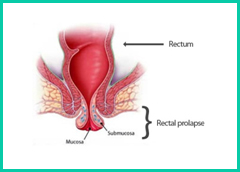
Full-Thickness rectal prolapse describes the entire rectum protruding through the anus- Mucosal prolapse describes only the rectal mucosa (not the entire wall) prolapsing
- Internal intussusception wherein the rectum collapses but does not exit the anus
The symptoms of rectal prolapse depend on the severity, but can include : -
- Pain and discomfort felt deep within the lower abdomen
- Blood and mucus from the anus
- The feeling of constipation, or that the rectum is never completely emptied after passing a motion
- Protrusion of the rectum through the anus
- The need to use huge quantities of toilet paper to clean up following a bowel motion
- Leakage of liquefied faeces, particularly following a bowel moti
- Faecal incontinence, or reduced ability to control the bowels.
Some of the symptoms may be the same: bleeding and/or tissue that protrudes from the rectum. Rectal prolapse, however, involves a segment of the bowel located higher up within the body, while haemorrhoids develop near the anal opening
How is rectal prolapsed diagnosed?A doctor can often diagnose this condition with a careful history and a complete anorectal examination. To demonstrate the prolapse, patients may be asked to sit on a commode and “strain” as if having a bowel movement as this brings the prolapse in clear view and makes the diagnosis easy.
Rarely, a rectal prolapse may be “hidden” or internal, making the diagnosis more difficult. In this situation, an x-ray examination called a video-defecogram may be helpful. This examination, which takes x-ray pictures while the patient is having a bowel movement, can also assist the physician in determining whether surgery may be beneficial and which operation may be appropriate. Anorectal manometry or measurement of pressures in the anal canal and function of the sphincter muscles around may also be required in some patients. All patients require a flexible sigmoidoscopy or internal examination of the large bowel to exclude any other pathology.
How is rectal prolapsed treated ?
Although constipation and straining may contribute to the development of rectal prolapse, simply correcting these problems may not improve the prolapse once it has developed. There are different operations for the treatment of rectal prolapse.
Treatment depends on the age of the patient and the severity of the prolapse, but could include: Diet and lifestyle changes to treat chronic constipation: for example, more fruit, vegetables and wholegrain foods, increased fluid intake and regular exercise. This option is often all that's needed to successfully treat rectal prolapse in young children. In cases of mucosal prolapse, the structures are secured in place with surgical rubber bands.
Surgery is sometimes used to secure the rectum into place, performed through the abdomen or via the anus. One operation involves tethering the rectum to the central bone of the pelvis (sacrum). Another operation is to remove the prolapsed part of the rectum and to rejoin the bowel to restore near-normal bowel function.
While abdominal surgery may give better long term results, elderly patients may be advised to undergo surgical correction via the anus, since it is easier to recover from this procedure.
How is laparoscopic surgery conducted ?
The operation to treat the rectal prolapse may be carried out from the abdomen or from rectal side. The surgeon takes into account factors such as age of the patient, physical condition, extent of prolapse and the results of various tests while deciding which route and which operation to use for treatment. By and large, patients who are fit to have a general anaesthesia benefit from a laparoscopic rectopexy. This operation is performed under general anaesthesia. The surgeon passes a cannula (a narrow tube) into the abdomen in the region of the umbilicus. A telescope connected to a camera is passed inside the abdomen through the cannula. The camera is connected to a television monitor so that a magnified view of the patient’s internal organs appears on the screen. The surgeon and his team conduct the operation by observing the television screen. The surgeon then inserts other cannulas and passes long, thin instruments inside the abdomen through them. Using these instruments the lowermost part of the large intestine – the rectum is freed up from its attachments. The rectum is then straightened up so that the prolapse gets pulled up. The rectum is then fixed to the bone behind called sacrum either with a few sutures or often by fixing a piece of mesh (net) between the bone and the rectum. This causes the rectum to stay fixed in the new, elevated position and prevents it from sliding down again.
Types of SurgeryThe goal of all of the surgical techniques involved in correcting a prolapsed rectum is to attach or secure the rectum to a backside (or posterior) part of the inner pelvis. Surgery is performed through either the abdomen or the perineum.
Surgery through the abdomenIn Hospital
- Typically performed in younger or healthier people
- Type of abdominal surgery usually determined by severity of associated constipation
- Associated with higher morbidity rate than perineal approach but lower recurrence rate of prolapse
- Performed under general anesthesia
- Usually involves a hospital stay of 3-7 days
Perineal approach
- Typically performed in elderly people or people in poor health
- Approach for people who cannot tolerate general anesthesia
- Associated with higher recurrence rate than abdominal approach
- Usually involves short hospital stay
What happens after laparoscopic rectopexy ?
patient is allowed to have liquids within 6 – 8 hours of surgery and food the day after. The patient generally gets discharged within 48 – 72 hours of surgery and is prescribed a mild laxative for about a month so that he or she does not strain during bowel The movement.
What are the results of this surgery?A great majority of patients are completely relieved of symptoms, or are significantly helped, by the appropriate procedure. Success depends on many factors, including the status of a patient’s anal sphincter muscle before surgery, whether the prolapse is internal or external, the overall condition of the patient. If the anal sphincter muscles have been weakened, either because of the rectal prolapse or for some other reason, they have the potential to regain strength after the rectal prolapse has been corrected. It may take up to a year to determine the ultimate impact of the surgery on bowel function. Chronic constipation and straining should be avoided after surgery.
What are the advantages of a laparoscopic rectopexy?
- The main advantage is that any cut on the body is avoided as the procedure is performed through tiny hole.
- It is a painless procedure.
- Patient is fit the same day and can return to normal day to day activity the same day.
- The time required for would healing is about 7 days in open technique which is completely avoided with the Laparoscopic gallbladder surgery.
- Complications like infection and scar can be avoided with laparoscopic technique
- Reduced surgery time.
- Only disadvantage is that cost of the surgery is about 30% higher than the open technique.
- Patient might require to convert to open method if any other complications are found during the surgery.
Complications
Some of the complications of rectal prolapse include : -
- Risk of damage to the rectum, such as ulceration and bleeding
- Risk of damage to the rectum, such as ulceration and bleeding
- Incarceration, which means the rectum can't be manually pushed back inside the body
- Strangulation of the rectum, which means the blood supply is reducedy
- Death and decay (gangrene) of the strangulated section of rectum.


