
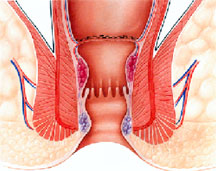
An anal fissure is a small tear in the skin lining on opening of anus. They are developed by hard or difficult bowel movements, causing severe itching, pain or bleeding. Your doctor Soumitra Chandra may recommend few changes in diet for soft stools and topical anesthetics to reduce pain. In case, surgery is required, Doctor Soumitra will work to relax the anal area so that there is less anal pain. Fissures can extend upward into the lower rectal mucosa; or extend downward causing a swollen skin tag to develop at the anal verge, also known as a sentinel pile.
Causes of Fissures
The most common cause of an anal fissure is injury to the skin at the anal opening due to a hard, dry bowel movement. Other causes include Diarrhea, Digital insertion (during examination), Foreign body insertion or Anal intercourse. With diarrhea, this condition is usually caused by an over use and over-wiping of an inflamed anal canal. Pregnant women may also develop a fissure during childbirth. They may be acute (recent onset) or chronic. Chronic fissures recur frequently or are present for a long time and are often associated with a small external lump called a skin tag or sentinel pile.
Symptoms of Anal Fissure
Severe pain is the main symptom of acute anal fissure. Fissure produced pain at defecation may persists for hours. A small amount of bright red blood, which may or may not be mixed with stool, is common. A fissure produces pain disproportionate to its size. An inadequately treated fissure may lead to chronic fissure in which pain is relatively less and persists intermittently for weeks and months.
How is Fissure diagnosed?
Diagnosis can be made by inspection. Closer inspection will frequently reveal a tag or sentinel pile. After gentle separation of the skin of the anal verge, the ulcer usually posterior can be seen. Frequently the fibers of the internal anal sphincter muscle can be seen at the base of this punched-out ulcer. A well-lubricated finger with lidocaine ointment and a small caliber anoscope will help delineate the extent of the lesion. A colonoscope or sigmoidoscope exam might be useful to rule out abscesses, colitis and other causes of rectal bleeding. A fissure should be distinguished from an ulcer caused by Crohn's disease, leukemia, or malignant tumors, because it is not shaggy, large or indolent. Fissures are seldom multiple. A biopsy can help to determine the diagnosis.
Treatment Options for Fissures
Medical treatment : A Conservative Management
At least 50 percent of fissures heal by themselves without the need for an operation. The longer that a fissure has persisted over time, the less likely it will be to heal by itself. Oftentimes, acute fissures heal by themselves spontaneously, with good anal hygiene consisting of a thorough cleansing after each bowel movement. The use of sitz baths (soaking the anal area in plain warm water for 10 to 20 minutes, several times a day) helps to relieve fissure symptoms, but may not actually aid in the healing process. A topical hydrocortisone preparation applied to the folds of the anal verge several times a day will help to relieve symptoms and aids the healing process.
A dietary modifications (i.e. incorporating a high fibre-well balanced diet and avoiding foods that are not well digested like maida, popcorn, chips), encouragement of regular normal stools, drinking plenty of fluids and using stool softeners/ laxatives are important in helping to heal the fissure. If pain is severe, an anesthetic ointment can be introduced freely and frequently with the finger, utilizing finger cots.
Chemical sphincterotomy has been attempted using a wide range of agents, including nitric oxide and botulinum toxin. Since anal fissures are characterized by spasm of the internal anal sphincter and a reduction in mucosal blood flow, the aim of treatment is to relieve ischemia by reducing resting anal pressure and improving mucosal perfusion.
It has been shown that a local application of topical nitrates reduces anal sphincter pressure and improves anodermal blood flow. This dual effect results in fissure healing in more than 80% of patients. The principal side effect is headaches in 20%-100% of cases.
It has also been shown that a local injection of botulinum toxin near the fissure, causes denervation, sphincter muscle weakness, and reduction of resting anal sphincter pressure, which allows the fissure to
heal. Fissure healing occurs in more than 60% of patients. The principal side effect is incontinence of flatus and or feces, which last for up to two months in 2% to 21% of cases.
Surgery : Surgery is used for treatment when fissures do not respond to other treatment. The two options available are:
Chemical Internal Sphincterotomy : A minimally invasive approach to relax the anal muscle by injecting chemicals in the anal sphincter muscle and partially paralyzing it.
Lateral Internal Sphincterotomy : In this surgery, a portion of the anal sphincter muscle is divided which helps the fissure to heal and decrease the pain and spasm. If a sentinel pile is present, it is removed to promote healing. It is a quick surgical process and can also be performed as a short outpatient procedure. The chances of recurrence are almost nil. It is the most effective treatment option for non healing fissures.
Piles (Conventional & Stapler Surgery)
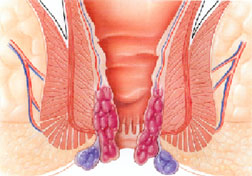
Piles are also called haemorrhoids. Hemorrhoids are masses, clumps, cushions of tissue in the anal canal and are full of blood vessels, support tissue, muscle and elastic fibers. They are classified into two general categories: Internal and External.
Internal Haemorrhoids lie far deep inside the rectum where you can't see or feel them. Due to the pain-sensing nerves in the rectum, they usually do not hurt. However, bleeding is the only sign of their existence.
External Haemorrhoids lie within the anus and are often uncomfortable. If an external haemorrhoid prolapses outside (usually in the course of passing a stool), you can see and feel it.
Causes of Piles
Piles develop due to chronic constipation that leads to excessive straining, resulting in swelling of veins in the rectal area. Pregnant women may also develop piles due to increased pressure on the veins in the pelvic area. There are some evidences that piles run in families.
What are the symptoms of Piles? Pain or ache around the anus and lower bowel (rectum), which can be really quite severe.
Pain or ache around the anus and lower bowel (rectum), which can be really quite severe.- There may be itching of the area especially after passing motions.
- There may be bleeding from the back passage. This will be bright red blood, not usually mixed in with the motion, but often seen on the toilet paper.
- There is often a feeling of something coming down, or a bulge or lump at the anus.
- If a haemorrhoid at the outside of the anus gets a blood clot in it (thrombosed external pile) it leads to a particularly tender, hardish lump.
Treatment Options for Piles
Physical examination and proctoscopy are done to diagnose piles. Dr. Soumitra may want to feel inside the anus with a gloved finger. Sometimes he will look inside with a metal instrument. This enables him to confirm the diagnosis, and to rule out other, more serious problems such as cancer.
In the early stages, piles resolve on their own and do not require any treatment. However, right treatment can significantly reduce the discomfort and itching that many patients experience. The treatment options available are as follows:
-
Depending on the diagnosis, the doctor advises whether you require home treatment or further intervention. Lifestyle and dietary modifications such as regular physical exercise, avoiding being overweight, plenty of fluids and a high fibre diet can provide symptomatic relief.
-
Surgery: Surgery is used for particularly large piles. Generally, surgery is used when conservative treatment/management is not effective. Sometimes surgery is done on an outpatient basis - the patient goes home after the procedure.
Surgeries for Piles
Haemorrhoidectomy (open surgery of the piles): In this procedure, the excess tissue that is causing bleeding is surgically removed. It may involve a combination of a local anesthetic and sedation, a spinal anesthetic, or a general anesthetic. This type of surgery is effective in completely removing piles, but can cause pain for few days.
In Open Method (Milligan-Morgan Technique), the bunch of dilated veins (piles) in the lower part of anal canal are dissected and then tied off. In order to avoid stenosis, three pear-shaped incisions are left open, separated by bridges of skin and mucosa. The dissection results in to a wound in the lower anal canal, which takes time to heal. Since the lower part of anal canal is highly sensitive to pain, the patient experiences agonizing pain for 4-5 post operative days. Therefore the patient is kept admitted in the hospital for 3-5 days. Normally the patient resumes work after 2-3 weeks when the wound is at least partially healed. The patient also needs to do hot water baths( Sitz bath) 2-4 times a day till the wound heals completely which usually takes 4-6 weeks.
Minimally Invasive Procedure for Hemorrhoids (MIPH) or Stapler Technique : MIPH is a technique developed in the early 90's that reduces the prolapse of hemorrhoidal tissue by excising a band of the prolapsed anal mucosa membrane with the use of a circular stapling device In this technique, the pile mass is not directly operated or dissected. Instead the operation is done in the upper anal canal which is insensitive to pain. A disposable Stapler device is used which cuts the lining of the anal canal and sutures it back instantaneously. In the process, the blood supply to the pile mass is obliterated and this results in shriveling and hence disappearance of piles. Moreover the excess tissue is removed which corrects the mucosal prolapse and restores the hemorrhoidal tissue back to its original anatomical position.
Since this operation doesn’t create any wound, the patient needs no post operative dressings and hot water baths( Sitz bath). As the lower sensitive anal canal is not cut during this procedure, the patient is absolutely pain free right after the operation and therefore can resume work the very next day. Moreover the time taken for operation ( 15-20 minutes) and the blood loss in Stapler technique is comparatively much less.
Before treatment After treatment
Few of its advantages are:- Minimal postoperative pain
- Shorter hospital stay
- Quicker recovery and return to normal activities
- Excellent cosmetic outcomes
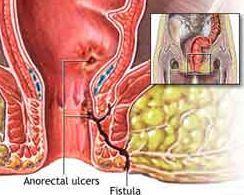
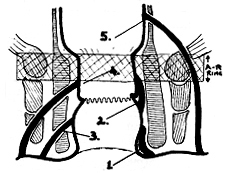
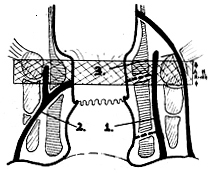
Anal Fistula / Fistula in Ano
Anal fistula is an abnormal track (lined by granulation tissue) connected between the anal canal or rectum and the peri-anal skin. Usually results from anorectal abscess due to blocked infected anal glands lying between the two layers of anal sphincters.
-
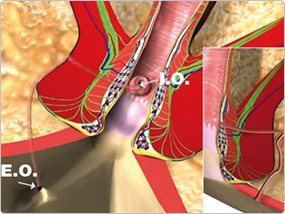
Normally anal glands drain into anal canal.
- If outlet of these glands is blocked, this results into abscess and eventually point out to skin surface.
- Tract formed by this process is a fistula. Rarely, the fistula may communicate from anus (rectum) to Vagina (Recto-Vaginal Fistula), Urinary Bladder (Recto-Vesical Fistula), Urethera (Recto-Uretheral Fistula) or other pelvic structures, including the bowel.
- If the track does not communicate with anal canal then it is called a sinus.
- Abscess can reoccur if fistula seals over, allowing the pus to accumulate and points to surface again and the process repeats.
Why is Anal Fistula such a dreaded (feared) disease? Is it really dangerous?
Anal Fistula is a dreaded disease. This is basically for three reasons :
1. If the treatment is not done, the pus inside the fistula can spread further leading to formation of multiple tracts and several opening in the skin around the anus. This makes the fistula more complex and further difficult to treat.
2. Anal Fistula treatment is associated with high recurrence rate. A lot of patients who get themselves operated by routine surgeons have to undergo multiple operations to get cured. The lure of curing this disease without operation by quacks further complicate the treatment. Therefore, Anal Fistula should always be treated by an expert Colo-Rectal Surgeon like Dr. Soumitra Chandra who is proficient in dealing with Anal Fistulas.
3. Another important issue is that many surgeons are used to /comfortable doing a particular procedure for Fistula. They do the same procedure in all the patients. There are 5-6 procedures to treat Anal Fistulas and none of these procedures is perfect. Therefore, different procedure should be done in different patients, depending upon the type and complexity of that patient's fistula. A single procedure cannot and should not be done in all the procedures. Very few surgeons are expert in doing all the procedures of Anal Fistulas like Dr. Soumitra.
4. There is a risk, though low, of cancer formation in the long standing Anal Fistulas. Therefore, Fistulas should always be treated at the earliest.
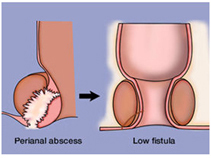
Most fistulas begin as anorectal abscesses. When the abscess opens spontaneously into the anal canal (or has been opened surgically), a fistula may occur. Approximately, 8-50% of perianal abscess patients end up having an anal fistula.
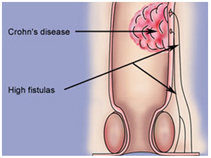
Other causes of fistulas include Tuberculosis, Cancer, Injury (trauma), Crohn's disease, Post radiation therapy, Anal Fissure and infections (actinomycoses, chlamydial, etc). Fistulas may occur singly or in multiples.
Anal fistulas most commonly develop as a result of an anal abscess. An abscess is a collection of pus and infected fluid. An anal abscess normally develops after a small gland, just inside the anus, becomes infected with bacteria or foreign matter. Abscesses are usually treated with a course of antibiotics. In most cases, you will also need to have the infected fluid drained away from the abscess.
If an anal abscess bursts before it has been treated, then it can sometimes lead to an anal fistula. A fistula may also occur if an abscess has not completely healed, or if the infected fluid has not been entirely drained away. An abscess does not always develop into a fistula. Approximately half of all people who experience an anal abscess will go on to develop a fistula. There is no way of predicting when a fistula will develop.
Anal fistulas are also a common complication of conditions that result in inflammation of the intestines. Some of these conditions include : -
-
irritable bowel syndrome (IBS)
- diverticulitis
- ulcerative colitis
- Crohn's disease
- tuberculosis
- gonorrhoea,
- cancer of the rectum.
The symptoms of an anal fistula may include : -
- a throbbing, constant pain
- irritation of skin around the anus
- fever
- evidence of pus or blood when passing stools
- generally feeling unwell.
Pain tends to worsen when you sit, move around, pass stools or cough. If a fistula has been caused by a condition which causes inflammation of the intestines, such as irritable bowel syndrome (IBS), ulcerative colitis, diverticulitis or Crohn's disease,
you may experience other symptoms such as : -
- abdominal pain
- diarrhoea
- loss of appetite
- weight loss
- nausea
- vomiting.
Types :
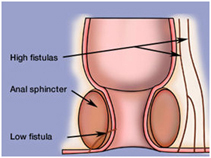
Divided into two groups depending upon their internal opening below or above the ano rectal ring
Low level – Open below the anorectal ring and have 5 varieties
High level – Open at or above anorectal ring and have 3 varieties
Standard Classification
Submucus
Subcutaneous
Low anal
High anal
Pelvi-rectal
Park’s Classification
Intersphincteric
Transsphincteric
Supralevator
The importance of knowing the type is that low fistula can be laid open without the fear of faecal incontinence while high fistula should only be treated in “staged” operations.
How is Anal Fistula diagnosed?-
Fistula probe.
- Anoscope[Proctoscope]
- Fistulography.
- Endo anal Ultrasound
- Magnetic resonance imaging
Treatment
Hall mark of treatment of fistula is to :
- Close the internal opening
- Take care of tract
- Not to damage the sphincters
- stop recurrence
VAAFT (Video assisted anal fistula treatment)
This technique is recently developed by Prof.Meinero, an Italian colorectal surgeon.
The main advantage of this technique is that every step is done under vision.
- 3mm Fistuloscope inserted through external opening.
- Track is dilated with pressurized glyceine solution.
- With gradual left to right, up or down movements follow the track.
- Identify & reach the internal opening .
- The whole track is coagulated with monopolar cautery cm by cm.
- Fistula pathway appears as charred filled with dark necrotic material.
- Necrotic material is removed under vision with fistula brush.
- Few sutures applied to close the internal opening .
- Lift the internal opening with the help of sutures like volcano/tent.
- A contour stapler or liner stapler is applied and the base of volcano which completes mechanical cutting and suturing.
Final results is small scar at the site of internal opening.
Finally, cyanoacrylate or fibrin glue is injected through external opening into the fistula pathway by a specific catheter to ensure hermetic closure of fistula.
It’s perfect excision and closure of internal opening.
- Day care surgery
- No surgical wounds
- No dressings required
- Accurate localization and closure of internal opening
- Fistula tract is completely destroyed
- No need to know if fistula is high/low
- No faecal incontinence
- No pain
- No medication required more than 7 days
- Can go back to work within 48 hours
- Economical
Several other options are
Doing nothing : This is the safest option in many inoperable cases although it does not definitely cure the fistula.
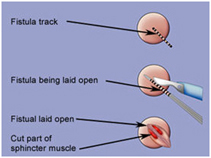
Lay open of fistula (Fistulotomy / Fistulectomy) :
- The whole track is laid open
- Requires daily dressing for 8-12 weeks
- Leaves behind scar
- Depending upon the position can cause incontinence problems
- Not suitable for fistula crossing the sphincters
Cutting Seton
-
Most suitable for high level fistula
- Done by inserting a tube through fistula track and tying it outside the body
- Requires tightening from time to time
- Takes very long
- Low risk of incontinence
Cutting Seton
- Most suitable for high level fistula
- Done by inserting a tube through fistula track and tying it outside the body
- Requires tightening from time to time
- Takes very long
- Low risk of incontinence
Fistula Plug
- Involves plugging the fistula with a device made from gut submucosa
- Positioned inside anus with sutures
- Stimulates body to close the fistula from the inside out
- Hospitalization for 24 hours
- No risk of bowel incontinence
- Not well accepted due to recurrence and rejection
Fibrin Glue Injection
- Being tried, with variable success
- Involves injecting biodegradable glue into fistula
- Minimal stress
- No risk of incontinence
Endorectal Flap Advancement
- Internal opening is identified and a mucosal flap cut
- around it
- Flap lifted to expose the fistula and the internal opening is sewn
- Flap is pulled over down the sewn internal opening and sutured in place
- External opening cleaned and sutured
- Variable success rates
Lift Technique
- It is ligation of intersphincteric fistula tract based on secure closure of internal opening and removal of infected tissue through intersphincteric approach. It includes incision at intersphincteric grove, identification of intersphincteric tract
- Ligation of IS tract close to internal opening
- Removal of IS tract
- Scarping granulation tissue from rest of tract
- Suturing the defect at external sphincter muscle
- Technically difficult
- Success rates as with as 94%
Perianal Abscess/ Perianal Fistula
A perianal abscess is (simply) a collection of pus, outside the anus. Infection of an anal fissure, sexually transmitted infections, and blocked perianal glands are all thought to be inciting factors. The abscess usually begins when bacteria enters through a tear in the lining of the rectum or anus. Most often, this occurs between the internal and external sphincters (intersphincteric abscess), where the perianal glands are located. As the abscess increases in size, most will follow the plane of least resistance and spread towards the surface, creating a perianal abscess.
Swelling around the anus and a constant, throbbing pain are the most common symptoms. Pain with bowel movements may be severe.
Other symptoms may include:
- Painful, hardened tissue
- Lump or nodule, swollen, red, tender at edge of anus
- Discharge of pus from the rectum
- Fatigue and general malaise
- Fever, night sweats, and chills
- Constipation
To treat an abdominal abscess, the pus must be drained, either by surgery or by a needle inserted through the skin. To guide the placement of the needle, a doctor uses CT or ultrasound scanning. Antibiotics are usually used in conjunction with drainage to prevent the infection from spreading and to help completely eliminate the infection. Complications may include:
- Peritonitis stops the movement of bowel contents (peristalsis), which can block the bowel (paralytic ileus).
- Septic shock – Fluid from the blood accumulates in the abdominal cavity and the loss of fluid from the circulation may also cause shock.
- Abscess
- Intraperitoneal adhesions
Symptoms
- Unable to sit comfortably
- Difficulty or pain with passing stool
- Redness or pain around anus
- Abscess felt around anus or within anal canal
- Peri-rectal swelling
- Pain may be throbbing, sharp, or dull
- Fever may be seen in severe case
- Bleeding or discharge if abscess is drained or accidentally ruptures.
- In elderly there maybe no fever only lower abdominal pain
- If the abscess ruptures and leaves a fissure that opens into the anal canal, a fistula is formed.
Causes
Bacteria :
- Staphylococcus
- E. coli
- Streptococci
- Proteus vulgaris
- Pseudomonas aeruginosa
- Bacteroides
- Usually a mixture of above
How the diagnosis is made
-
Need examination by a doctor
- If abscess is in the canal, the doctor may need to insert his gloved index finger in the canal (digital rectal exam) and feel for it.
- If fever is present and the patient appears sick, blood samples may be taken to assess the severity of infection.
- Barium Enema -- an enema used to pour a chalky substance called barium through the anus into the rectum for X-raying. This will help if the abscess cannot be felt, or if a fistula is present.
- Sigmoidoscopy -- a rigid tube inserted into the rectum allows the doctor to look inside.
The operation
You will have a general anaesthetic, and will be asleep for the whole operation. The pus is let out through a cut in the skin. The surgeon will also wash out the area of the infection to minimise the chances of it coming back. The wound is packed with swabs. Antibiotics are given to help the healing. You should be able to go home after one or two days. For the first week or so after the operation, the swabs are changed for clean ones about every other day.
This can be done on the ward while you are in the hospital under the supervision of Dr. Soumitra Chandra or in the outpatients clinic. After that you will not need any more swabs in the area and at about a month later the wound is examined to see if any more treatment is needed.
If you let nature take its course, the abscess will discharge pus after several days. While you are waiting, you will have a lot of pain and a high temperature. The abscess will get much bigger than if you had it drained. Healing will take much longer. You will be off work and off colour for much longer. There is a considerable chance that the abscess can spread and you could end up with a generalised infection (sepsis) which could be potentially lethal. Antibiotics have not worked for you. Heat treatment and ointments will not help.
Before the operationStop smoking and get your weight down if you are overweight. If you know that you have problems with your blood pressure, your heart, or your lungs, ask your family doctor to check that these are under control. Check Dr. Soumitra's advice about taking the Pill or hormone replacement therapy (HRT). Check if you have a relative or friend who can come with you to the hospital, take you home, and look after you for the first week after the operation. Sort out any tablets, medicines, inhalers that you are using. Keep them in their original boxes and packets. Bring them to the hospital with you.
On the ward, you will be checked for past illnesses and will have special tests to make sure that you are well prepared and that you can have the operation as safely as possible. Please tell the nurses of any allergies to tablets, medicines or dressings. You will have the operation explained to you and will be asked to fill in an operation consent form.
Before you sign the consent form, make sure that you fully understand all the information that was given to you regarding your health problems, the possible and proposed treatments and any potential risks. Feel free to ask more questions if things are not entirely clear to you.
There is some discomfort on moving rather than severe pain. You will be given injections or tablets to control this as required. Ask for more if the pain is not controlled or if it gets worse.
A small computer controls the amount of painkiller that is released and prevents any accidental overdose. Alternatively, you may have a fine tube in your back through which pain relief can be given to help control the pain. A general anaesthetic will make you slow, clumsy and forgetful for about 24 hours. The nurses will help you with everything you need until you are able to do things for yourself. Do not make important decisions, drive a car, use machinery, or even boil a kettle during this time.
You will most likely be able to get out of bed with help of the nurse the day after operation despite some discomfort. You will not do the wound any harm, and the exercise is very helpful for you.
You may be given a blood-thinning injection in your skin once a day to prevent any blood clots in your legs. This can happen in the first few days after the operation until you can move around a bit more. Those clots can be very dangerous because they can 'travel north' through your blood stream to your heart and lungs and cause very serious problems and even death. You should be comfortable enough to go home within one or two days.
The first time you open your bowels it may be a bit painful but this should improve over time. It is important that you pass urine and empty your bladder within 6 to 12 hours of the operation. If you find using a bed pan or a bottle difficult, the nurses will assist you to a commode or a toilet. If you still cannot pass urine let the nurses know and steps will be taken to correct the problem. You may need a catheter (fine plastic drain tube) put in your front passage to drain the urine from your bladder until you are able to pass urine comfortably on your own.
The wound has a dressing held on by elastic netting pants. There may be some staining with old blood during the first 12 hours. The dressings will be removed the day after operation and will be replaced with a lighter dressing.
There may be stitches in the wound. You can wash as soon as the dressings have been removed but try to keep the wound area dry for the time (about a week) you will have swabs in the wound. Soap and tap water are entirely adequate. Salted water is not necessary. You may be given an appointment to visit Dr. Soumitra for a check up one week after you leave hospital. Any stitches will be taken out at this visit. The nurses will advise about sick notes, certificates etc.
You will be given dressings to use at home as needed. You will be given a supply of antibiotics. You may be uncomfortable for three to four days. The wound should heal within two weeks. You can drive as soon as you can make an emergency stop without discomfort in the wound, i.e. after about 10 days.
You can restart sexual activities within a week or two, when the wound is comfortable enough. You should be able to return to a light job after about one week, and any heavy job within two weeks.
- As with any operation under general anaesthetic, there is a very small risk of complications related to your heart and lungs. The tests that you will have before the operation will make sure that you can have the operation in the safest possible way and will bring the risk for such complications very close to zero.
- Complications are relatively rare and seldom serious. If you think that all is not well, please let the doctor Soumitra or nurses know. The wound is always a bit moist for a week or two. There is likely to be a discharge of yellow matter and even some dark blood on the dressings during this time. Opening your bowels will rapidly become easier, particularly if you take a laxative. DO NOT however take bran or a high-fibre diet until the back passage is pain-free in case you end up with a blockage.
- There is a very small chance that you may experience some persistent bleeding after the operation or, even more rarely, there is chance that some damage will be caused to a vessel, a nerve or your back passage during the operation. In a situation like this you will need another operation to fix the problem.
- There will be greater chance of complications if the operation is delayed, however every effort will be made to reduce any such risk.
- The operation to drain the abscess solves the problem completely in just over 50% of cases. In the remaining patients a small permanent communication (fistula) can develop between the back passage and the skin with recurrent local infection, which can, in some people (like the elderly or diabetic patients) develop into an abscess again. If this is the case you will probably need another operation correct the fistula between the back passage and the skin.
Gastrointestinal Oncology Surgeon Dr. Soumitra Chandra is always dedicated to preventing, diagnosing, treating, and managing cancers of the gastrointestinal system (also called the digestive system). These include cancers of the rectum, anus, pancreas and stomach. The specialized approach of Dr. Soumitra Chandra to treating gastrointestinal cancers provides patients with the exact type of services they need to battle their specific disease and its physical, emotional and social side effects.
Surgery for Colo Rectal CancerIntroduction:
Colorectal cancer is common in developed countries such as the USA and Japan, and lower in frequency in developing countries like Africa and Asia. The incidence is slightly higher in men than women, and is highest in African American men. Colon and rectal cancer is the third most common cancer in both women and men in the US.
Symptoms
Though not specific but there are warning signs like bleeding in stools, sensation of incomplete passage of stools, feeling of bloating or obstruction in intestine, unusual loss of weight and fatigue, alteration of bowel habits, blood and mucus in stools.
Causes
- If your diet has high fat content and low in fibers,
- fruits and vegetables
- If you have a close relative with cancer of colon and rectum
- If you have colonic polyps
- If you have inflammatory bowel disease like ulcerative colitis, crohn’s disease
- Familial polyposis syndromes
- Age more than 50 years
Prevention :
No specific intervention for primary prevention is known. However, the following dietary and lifestyle changes may play a role in prevention :
- physical activity
- folate
- fruits and vegetables
- calcium
- vitamin D
- high fiber diet
- weight reduction
- avoidance of red and processed meat
- stopping smoking.
For secondary prevention, 2 broad groups have been identified :
a. High risk individuals (those with a history of adenomas or cancers, family history or genetic syndrome, or inflammatory bowel disease). Among the high risk groups a colonoscopy should be done 3 years after removal of an adenoma/polyp and if this is normal then after 5 years the test should be conducted.
b. Average risk individuals (all others)
Diagnostic tests?
History: Rectal bleeding is the commonest symptom. Other symptoms include tenesmus, altered bowel habits and mucus discharge, weight loss and loss of appetite.
For suspicious or high risk patients the best diagnostic tool is sigmoidoscopy or colonoscopy. These are endoscopies done through anal route to visualize the entire large intestine from inside. When colonoscopy is not possible other test recommended is Barium enema or CECT scan. USG, X Rays of Abdomen are the other tests recommended during diagnosis and staging the colorectal cancers.
Treatments of colorectal cancers?
Surgery, chemotherapy and pre-operative Radiotherapy (short course or long course) are used in the treatment protocol of colon rectum in different sequences depending on stage of disease. Out of these surgeries these are the primary treatment and curative treatment required in early stages.
What should patients know before surgery?
- What kind of operation will it be?
- How will I feel afterward? If I have pain, how will you help me?
- Will I need a colostomy? Will it be temporary or permanent?
- How long will I be in the hospital?
- Will I have to be on a special diet? Who will teach me about my diet?
- When can I return to my regular activities?
- Will I need additional treatment?
Surgery for Pancreatic Cancers
Introduction
Pancreas is a organ located on back side of abdomen behind stomach. Actually this is an active gland responsible for digestion of food and secrete Insulin for control of blood sugar. Acute pancreatitis is an important cause of acute upper abdominal pain associated with vomiting. The common causes include gall bladder stone disease, alcoholism and idiopathic- where no obvious cause is discernible. Fortunately the majority of cases of acute pancreatitis are mild and respond to conservative treatment. In less than 10% the disease is more severe and follows a vicious course with immense clinical and socio economic implications.
Causes and Risk factors for Cancer of Pancreas
- Age more than 50 years and male preponderance is often seen
- Cigarette smoking
- Heavy alcohol consumption
- Diabetes Mellitus
- Diet high in fat and protein contents
- Chronic pancreatitis
- Family history of cancer of pancreas
Prevention
In a known case of alcohol induced pancreatitis the patient must be counseled about the role of alcohol and that abstaining from it will prevent a further episode of pancreatitis. Similarly avoidance of fatty food and early cholecystectomy in a known case of biliary or gall stone induced pancreatitis will prevent further attacks.
Cancer Detection Test
After detailed history, examination and routine tests Dr. Soumitra will advice certain specific tests like liver function tests, USG, CECT abdomen, MRCP, CA 19.9 or PET Scan if required.
Treatment Procedure
Treatment depends on the stage and fitness of the patient. Surgery is the mainstay in this cancer particularly in early stage. The type of surgery depends on the location of tumor whether they are in head or body or tail of pancreas. It also depends on whether they have involved other surrounding organs or blood vessels. If they aren’t wide spreaded then localized surgery always have the potential for cure. Radiotherapy and chemotherapy is also employed either for unresectable tumors or after surgery for tumors which were not in very early stage.
What to do if tumor is not resectable?
Sometimes surgical removal of tumor is not possible ( locally advanced tumors with involvement of other organs or important blood vessels ) or not advisable ( due to dissemination of cancer ). In these situation cancer can be down staged by chemotherapy and Radiotherapy in certain percentages of patients and then operated. Otherwise they can be given the opportunity of selecting bile duct and /or Duodenal stenting or Triple bypass ( surgical method of bypassing the obstructed ( blocked ) bile duct and duodenum.
Introduction
Stomach Cancer represents the fourth most common malignancy and the second leading cause of cancer related death. In Japan gastric cancer remains the most common type of cancer among men. Its incidence, however, has been declining globally since World War II. Gastric cancer is one of the least common cancers in North America. The incidence of proximal gastric cancer is on the increase while the distal gastric cancer is declining in North America. The five year survival rate of gastric carcinoma is low (10-20%).
What is Stomach Cancer?
The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive system, which processes nutrients (vitamins, minerals, carbohydrates, fats, proteins, and water) in foods that are eaten and helps pass waste material out of the body. Food moves from the throat to the stomach through a hollow, muscular tube called the esophagus. After leaving the stomach, partly-digested food passes into the small intestine and then into the large intestine. The wall of the stomach is made up of 3 layers of tissue: the mucosal (innermost) layer, the muscular is (middle) layer, and the serosal (outermost) layer. Gastric cancer begins in the cells lining the mucosal layer and spreads through the outer layers as it grows.
Gastric Cancer refers to the malignant growth arising from the epithelial lining of the stomach. It is an aggressive tumor with vague early symptoms and spreads to the adjoining structures early in its course. Stromal tumors of the stomach begin in supporting connective tissue and are treated differently from gastric cancer.
Causes of Stomach Cancer
Vast majority of Gastric Cancers are attributed to environmental factors, the most common being infection with Helicobacter Pylori. This organism has been found in almost 70% of the patients with Antral gastric cancer and is associated with nine fold increased risk of developing gastric cancer. Inoculation most likely occurs in childhood through the oro-fecal pathway and is transmitted from person to person.
Intake of certain food contents is also thought to be contributory; preserved diets with high salt contents, smoked foods and diets with low fresh fruits and vegetable contents have also been attributed to the increased incidence of gastric cancer.
Smoking and prolonged consumption of alcohol have also been attributed to the increased occurrence of gastric cancer. Better living standard, better dietary habits, eradication of Helicobacter Pylori infection, giving up of smoking and alcohol consumption may decrease the occurrence of gastric cancer.
1-3% of gastric cancers are associated with inherited gastric cancer predisposition syndromes. E-cadherin mutations occur in approximately 25% of families with an autosomal dominant predisposition to diffuse gastric cancers also called hereditary diffuse gastric cancer. This subset of persons may benefit from genetic counseling and prophylactic gastrectomy.
Types of Surgery :
Multi-disciplinary treatment planning is mandatory for a better outcome of this rather dismal disease. Patients with Gastric cancer should be managed by an experienced team of Surgeons, Onco-physicians, Gastroenterologist, Radiation-Oncologist, Nutrion Specialist and Onco–Nurses.
Surgery remains the mainstay of treatment of gastric cancer. It is the only single modality treatment capable of curing the disease. The goal of surgical cure requires complete resection.
Subtotal (partial) gastrectomy:
This type of surgery is often used by some of the best cancer hospitals in India if the cancer is only in the lower part of the stomach close to the intestines. It is also sometimes used for cancers that are only in the upper part of the stomach. Only part of the stomach is removed, sometimes along with part of the esophagus or the first part of the small intestine. Eating is much easier after surgery when only part of the stomach removed.
Total gastrectomy:
This method is used if the cancer has spread throughout the stomach. It is also often used if the cancer is in the upper part of the stomach. The surgeon removes all of the stomach. The nearby lymph nodes are removed, and sometimes also the spleen and parts of the esophagus, intestines, pancreas, and other nearby organs. The end of the esophagus is then attached to part of the small intestine. People who have had a total gastrectomy can only eat a small amount of food at a time. Because of this, they must eat more often.
Side Effects of Surgery?
Surgery for stomach cancer is complex and can lead to problems. These could include bleeding from the surgery, blood clots, and damage to the nearby organs. Rarely, the new connections between the ends of the stomach and esophagus or small intestine may not hold together and can leak. These problems, which could be fatal, were more common in the past.
Other side effects may start after you have recovered from surgery these could include :
- Heartburn
- Abdominal pain
- Diarrhea (especially after eating)
- Shortages of some vitamins


